Everything You Need To Know About Cannabis
-From A Neuroscientist who is 98% un-biased
Morgan Levy, MD
Levystien Productions Parker, Colorado Copyright 2014 9,500 words
Contents
Section I
Introduction The story of Levy Thamba What is cannabisSection II
Somatic effects Psychiatric effects Cognitive effects DrivingSection III
Medical uses Pharmacology Biochemistry Research issuesSection IV
Legal issues Political issues Social issuesSection V
HempConclusion
Addendum:
How to safely consume cannabis.References
SECTION I
Introduction
The first thing I discovered when I began to research cannabis is that you can't believe anything that anyone says or writes about it. Few of the scientists, physicians, government officials, growers, users or political activists have an un-biased opinion. Everyone seems to have an agenda and ... my God ... do they stretch the truth or what?
One side says: Cannabis has no medical use and it causes individuals to become violent, it is a frequent cause of car accidents, it can destroy your soul, it is a gateway drug, it is more dangerous than cocaine, it is more addictive than heroin, it causes as much harm as alcohol, it is used by communists to control people, it can undermine the rule of law in a civil society, it makes white women vulnerable to being defiled by black men, it causes cancer, it causes lung disease, it causes heart disease, it causes insanity, and the efforts of the US government to prohibit the use and abuse of cannabis have been largely successful.
The other side says: Cannabis is non-addictive, has a minimal effect on driving ability, is not toxic, does not cause death, does not cause insanity, and it has 250,000 uses. It is a great medication for glaucoma, nausea, pain, poor appetite, cancer, diabetes, AIDS and 15,000 other illnesses. It has been around for thousands of years which means that it is a safe wonder drug. Furthermore, the Hearst and DuPont families conspired to make it illegal in order to protect the paper and plastic industry from competition with hemp. Hemp was outlawed due to racism. Hemp seeds are such a cheap and wonderful food source that they could end world hunger. Hemp is a major threat to the tobacco, alcohol, oil, and pharmaceutical industries. Hemp could save the planet by ending the cutting down of trees. Hemp could end war by replacing petroleum. Drug companies won't develop cannabis medicines for devious reasons. The government's attempt to get rid of it has failed miserably and last, but not least, George Washington smoked it so it must be OK.

On the second day of legalization here in Colorado there was this fictional news article produced by anti-cannabis folks that was widely quoted requiring numerous public officials to later apologize.
Marijuana Overdoses Kill 37 in Colorado On First Day of Legalization
Jan 02, 2014
Colorado is reconsidering its decision to legalize recreational pot following the deaths of dozens due to marijuana overdoses.
According to a report in the *Rocky Mountain News, 37 people were killed across the state on Jan. 1, (2014), the first day the drug became legal for all adults to purchase. Several more are clinging onto life in local emergency rooms and are not expected to survive.
*hint- The Rocky Mountain News closed its doors forever on Feb. 27, 2009.
·
The pro-cannabis folks do no better in regards to truth telling. Here is a seemingly factual list of good things about cannabis.
Business Insider
23 Health Benefits Of Marijuana
Jennifer Welsh and Kevin Loria April 20, 2014
Here is number 7 on this list:
THC slows the progression of Alzheimer's disease.
REUTERS/Brian Snyder
Marijuana may be able to slow the progression of Alzheimer's disease, a study led by Kim Janda of the Scripps Research Institute suggests. The 2006 study, published in the journal Molecular Pharmaceutics, found that THC, the active chemical in marijuana, slows the formation of amyloid plaques by blocking the enzyme in the brain that makes them. These plaques are what kill brain cells and cause Alzheimer's.
It would seem from this article that Alzheimer disease has been cured!
Unfortunately, we don't know if THC would cause amyloid to stop making plaques in a living human brain. All we can say is, "There may be an interaction between amyloid and THC in a rat model of Alzheimer disease."
Since rats don't get Alzheimer disease it would be more accurate to say, "an artificially simulated rat model of Alzheimer disease."
What the article actually says is that THC competitively inhibits the enzyme acetylcholinesterase (AChE) as well as prevents AChE-induced amyloid β-peptide (Aβ) aggregation, the key pathological marker of Alzheimer's disease. Yes, this aggregation causes plaques and there is a lot of mounting evidence to suggest that the plaques are associated with memory impairment but we don't know what causes the aggregation. We don't know if stopping the aggregation in a living human brain would slow the disease progression.In other words, this is a long way from a cure.
I need to see some convincing evidence before I give a dementia patient a drug that is sure to worsen their cognitive function. Whoever wrote this article even misspelled Alzheimer disease. There is no apostrophe "s." The disease was named after Alois Alzheimer but it does not belong to him.
The other 22 health benefits on the Business Insider list are similarly full of partial truths without full explanations.
"My kingdom for an article that has a modicum of scientific merit!"
Whatever are we supposed to think?
If anyone tries to tell you what to think about cannabis you should ask,
"Who is saying this and what is their agenda?"
Since I am going to tell you what to think about cannabis let me tell you who I am and what my agenda is. I am a 50 year-old geriatric psychiatrist and dementia researcher who has been disabled for 10 years due to multiple sclerosis. I smoked marijuana several times when I was in medical school and have not used it again until this month. I did not feel that the high was worth doing something illegal. I live in Colorado and plan on consuming legal cannabis in the near future. I have no personal agenda with regards to cannabis.
The only income I generate from writing this essay is the small amount I make off the random and revolving advertisements. I am not funded by any person or group. I do this in my spare time because I enjoy it and because I think it might be helpful.
I have friends who are heavy users. I have friends who are moderate users and I have friends who think it is the devil's medicine.
As a psychiatrist, I have treated numerous individuals who have substance abuse disorders including individuals who were having a cannabis induced brief psychotic episode. I have some entertaining stories you can ask me to tell you if we are ever sitting around smoking cigars and drinking rum together. For example, one time an old friend from high school that I had not seen in years was picked up by the Denver police because she was running naked in the street. She spent about 48 hours on our locked psychiatry unit. We had a wonderful conversation after she recovered from her brief psychotic episode.
Despite my lack of experience as an end user, I do have some experience as a treating physician and researcher. I understand medications and the approval process, the pharmaceutical industry, the biochemistry of the endocannabinoid system, pre and post synaptic receptor sites, inhibitory neurotransmitters, brain function, the pre-frontal cortex, and the developing brain. Also, I know how to do medical research. I am writing this essay in order to educate people about cannabis because of all the misinformation that is out there and the fact that lots of individuals who are naive users are suddenly using here in Colorado.
Hey, I have an idea. Since I am a naive user myself, why don't I take you along with me as I learn how to use cannabis. I have friends who are recreational users and I have invited them over to teach me how to use it. I will document the account of how that goes in this essay.
In regards to the issue of whether cannabis is good or bad for individuals and/or society, Colorado is now running an interesting experiment. To investigate it I have planned to go to a pot shop since they opened in January. It is now June and I have yet to go.
A friend and his wife came from California and they went. They gave me an e-cigarette and I took 8 or 10 hits and felt nothing. I had already been smoking a cigar and drinking rum. (very good rum, by the way...Zacapa XO...well, I digress) In any case, I fell asleep sitting on the floor of my living room.
I learned that you need to smoke cannabis without any other drugs in your system and start with just one or two hits. I also learned that there are numerous ways to consume it including bongs, pipes, hookahs, joints, one hitters, vaporizers, bubblers, and all sorts of edible products. These different ways of consumption can affect the onset and duration of action.
WEED SMOKING DEVICES
There are hundreds of strains of cannabis that have various different potencies and effects. Some wake you up and some put you down.
A friend who is a long term casual user said, "Neither the shops nor the dealer on the street can really tell you for sure what you are getting. The different strains have different names and these names seem to have some consistency across the board with respect to effects."
I asked, "What strain is your favorite?"
He said, "Alaskan Thunderfuck."
I replied, "OK ... that sounds like one that would have a bad outcome. What does it do for you?"
He explained, "It gives me a decent body high and a mild to moderate head high without immobilizing me."
(He gave me this strain and I tried it. I was a bit anxious but I did feel a mild "body" high. I did not think it was that great of a feeling. There was zero "head" high and I do not think I was impaired at all even though I eventually took about 7 or 8 hits over a 60 minute period. I certainly was not hallucinating.)
I asked, "If you purchase cannabis from a dealer instead of a shop do you get the same named strains?"
He said, "Yes, the potency might vary a bit but generally yes."
I began to think that this cannabis thing was going to be a lot more complicated than I thought. I wondered how all these naive users who are flooding to Colorado are going to deal with it. Then, I remembered that a naive user came from Wyoming a few weeks ago and things did not work out well for him.
The story of Levy Thamba
There were some young men from a college in Wyoming who decided to come to Denver for the purpose of legally purchasing and consuming marijuana. They went to one of the new pot shops that opened when the law took effect on Jan. 1, 2014. They purchased a cookie and were told to only eat one sixth of it. They were warned that eating more would result in an over-dose. They had heard multiple reports that nobody ever dies from a cannabis over-dose. They also expected the effect to be relatively immediate as this is what they knew from people who had smoked cannabis. When there was no effect after 30 minutes Levy decided to eat the entire cookie. He was unaware that when you consume cannabis by eating it the effect is delayed.
Levy (no relation) was a healthy young man who had many friends. They say that he did not do drugs and this was his first experience with cannabis.
After ingesting the overdose he became hostile and erratic. His friends calmed him down and after some time they went to bed. They were in bed for a while when Levy suddenly jumped up and ran out of their fourth floor room. He leaped over the balcony and plummeted four stories to his death.
When I heard what happened to Levy I realized that the state of Colorado had made little effort to educate anyone about cannabis. His story was not surprising to me at all. I have seen brief psychotic episodes that were induced by cannabis in the emergency room and on the acute locked psychiatry unit more than a few times. Cannabis in higher concentrations and/or in susceptible individuals can have this effect and naive users are especially prone. It seems that you need to have some practice being in an altered state of mind in order to be sure that you can cope with it. People who do cannabis frequently refer to these episodes as "bad trips." Even experienced users sometimes have them.
A cannabis induced brief psychotic episode resulting in death is not common but it happened twice in the same week here in Colorado. Cannabis is not nearly as dangerous as alcohol, tobacco, heroin, cocaine, or methamphetamine in regards to health issues but it is not a totally safe substance.
The State of Colorado, to their credit, quickly passed legislation that requires appropriate packaging and labeling on all edible forms of cannabis that are sold. I have not seen the new packaging but the old packaging only gives the number of milligrams or says nothing or is not packaged at all.
(There is an addendum at the end of this essay on how to safely consume cannabis.)
----------Warning----------
Beware of synthetic cannabis
David Mitchell Rozga shot himself in the head with a family owned hunting rifle in an apparent suicide on June 6, 2010. It was reported by friends that they had smoked K2 with Rozga approximately one hour before his death. On Nov. 16, 2013, Kurtis Hildreth dropped dead shortly after smoking Spice. On July 12, 2014, Connor Eckhardt also dropped dead shortly after smoking Spice. There are thousands of other users who have been made seriously ill. Synthetic cannabis also known as K2, Spice, fake weed, Yucatan fire, or Moon rocks has caused death secondary to inducing a brief psychotic episode and it has caused death directly. It first went on sale in early 2000 and was advertised as an herbal blend that was non-toxic. Laboratory analysis in 2008 showed that it contains synthetic cannabinoids that bind to endocannabinoid receptors in a manner similar to THC. It turns out that there are a number of designer cannabinoids that have been created in the laboratory and that these chemicals are routinely sprayed onto the herbal combinations that comprise a typical bag of K2 or Spice. These compounds are difficult to detect in blood tests and it is impossible to know what is in any particular bag of fake cannabis. K2 and Spice are also difficult to study because the makers change contents routinely. We know that individuals have had severe psychotic reactions and that death has occurred in young healthy individuals shortly after use. President Obama signed into law the Synthetic Drug Abuse Prevention Act of 2012. All synthetic compounds that mimic the effects of THC are now schedule I controlled substances and illegal to sell or posses in the US.----------------------------
What is cannabis?
When you go to the pot shop there will be jars that contain plant material for making a joint. They often have funny names on the jar but they may or may not have any indication of potency. The person behind the counter will tell you but, I mean, come on.
Usually, they will describe the effects of different named strains. For example:
Lemon Skunk X Maui Wowie is an indica strain that is highly potent. It is good for relaxing, sleeping, and forgetting things. Be careful because you might lay on the sofa for several hours unable to get up.
Maui Waui is a sativa strain that has medium potency. It will uplift you and provide energy and happiness. It will help with anxiety, depression and pain.
Alaskan Thunderfuck is a Hybrid Sativa/Indica strain with medium to high potency that works great for pain and appetite. It will also make you happy and energetic.
You can find reviews on most strains at these sites:
Search by desired effect: Medical Marijuana StrainsSearch by name of strain: LeaflyThe physician in me would like to tell you to purchase cannabis that is exactly 7.5% THC. This will not work at the pot shop. You will need to say something like, "I want some medium potency cannabis that will help with my pain and anxiety. I want to feel it in my body and I want a mild euphoria but do not want to be glued to the sofa." They will suggest several stains by name and describe the effects associated with each strain. Potency will be an estimate. That is how it is done.
The most common form of marijuana consists of the dried flowers and subtending leaves and stems of the female Cannabis sativa indica, Cannabis sativa sativa, or hybrid indica/sativa plant. Generally speaking, you can purchase cannabis with THC content up to about 24% or so. The higher content cannabis is referred to as "Skunk." I would suggest that you smoke cannabis that is less than 15% THC.
There are other forms of cannabis that are much higher in THC content. Kief is a powder, rich in trichomes, which can be sifted from the leaves and flowers of cannabis plants and either consumed in powder form or compressed to produce cakes of hashish. Hashish (also spelled hasheesh, hashisha, or simply hash) is a concentrated resin cake or ball produced from pressed kief. Cannabinoids can be extracted from cannabis plant matter using high-proof spirits (often grain alcohol) to create a tincture, often referred to as "green dragon." Hash oil is obtained from the cannabis plant by solvent extraction. Infusions are made when the plant material is mixed with a solvent and then pressed and filtered to express the oils of the plant into the solvent. There are many varieties of cannabis infusions owing to the variety of non-volatile solvents used such as cocoa butter, dairy butter, cooking oil, glycerin, and skin moisturizers. "Ear wax" is an extremely potent (up to 90% THC) form that is made with aerosol butane and the resin of the leaves and buds of the female plants. The result is a yellow-green waxy material.
I include these various forms and potency alerts due to the fact that people are often given a cannabis product without being accurately informed of its potency. Naive users are especially vulnerable. You should also inspect these forms prior to consumption as they may contain adulterants such as lead, heavy metals, or soap.
Hmmmmm .... well, so,
What is the real danger?
and
What are the real benefits?
I will now list every issue with regards to cannabis and provide a brief opinion. I have studied each of these issues extensively. I am using my most skeptical eye. I tried not to fall for logically fallacious arguments. I investigated all individuals whose names are on studies or who are making claims of any kind. I am presenting my opinion after a synthesis of a lot of contradictory information. It is virtually impossible for any human, myself included, to be without bias at all but I tried to be as objective as possible in this article.
SECTION II
All possible effects for all strains of cannabis are listed below but each strain will have its own unique subset of these effects.
Somatic effects
acute: Increased heart rate (tachycardia up to 20-50%), increased cardiac output, increased cerebral blood flow, decreased blood pressure (hypotension), dry mouth, red eyes, decreased intra-ocular pressure, bronchodilation, increased appetite due to decreased blood sugar (hypoglycemia), muscle relaxation, sensation of cold or hot feet, depressed motor activity, persistent lower frequency alpha waves on EEG, and rarely nausea, vomiting, diarrhea, and urinary retention.
chronic:
caveat- Long-term research on cannabis is un-reliable for several reasons. It has been illegal to obtain for study purposes so there have been few applications for grant funded research until very recently. Due to cannabis being an illegal herbal product that contains some 450 different constituents with 60 or 70 that are physiologically active there is no way to know exactly what an individual in an epidemiological study actually consumed. Unfortunately, most of the studies that we can site on cannabis are epidemiological. The small amount of data from controlled studies almost always used a THC extract that contained no other cannabinoids. The two FDA approved synthetic THC medications (Marinol and Cesamet) and the synthetic THC/CBD combo medication that should be approved soon (Sativex) have isolated constituents of cannabis and have undergone traditional phase I-III studies to get approval. For whatever reason, it seems that a lot of the effects are lost when these medications are compared with the herbal or botanical form. Finally, it is my opinion that most of the research is conducted by individuals who have a theoretical and/or financial bias about cannabis and have a desire to fulfill an agenda. Therefore, it is difficult to generalize from these studies.
Nevertheless, here is what we may or may not know.
Chronic low dose cannabis (3 or 4 drags of cannabis 3 or 4 times per week or less) has little toxic effect and may have some positive health benefit.
Chronic high dose cannabis produces negative health effects.
This would be similar to a glass of red wine with dinner having positive medical benefit but a bottle per day causing problems.
Chronic daily cannabis use over a number of years causes:
a. Lungs- bronchitis, tissue damage, and possible cancer
b. Bladder- possible cancer
c. Testes- possible germ cell cancer
d. Head and neck- possible cancer
e. Liver- possible cancer especially in individuals who have hepatitis C
f. Heart- Cardiac complications such as heart attacks may be induced by acute intoxication with cannabis due to tachycardia and hypotension. I believe that this is most likely to occur in individuals who have pre-existing cardiac pathology. It is unlikely that cannabis use directly causes cardiac disease but it may contribute to its development in long term heavy users.
g. Pregnancy- possible birth defects
Psychiatric effects
acute: Euphoria, feelings of well-being, talkativeness, giggling, carefree feeling, alteration of conscious perception, relaxation, stress reduction, increased appreciation of humor, ability to discern details of arts and music, joviality, metacognition, introspection, enhanced recollection (episodic memory), increased sensuality, increased awareness of sensation, increased libido or decreased libido, increased creativity, abstract and philosophical thinking, magical thinking, increased enjoyment of food taste and aroma, distortion of sense of time and space, altered body image, disruption of linear memory, pleasant auditory and/or visual hallucinations, ataxia, and occasionally dissociative states such as depersonalization and derealization. alternatively- cannabis can sometimes cause anxiety, panic attacks, paranoia, frightening hallucinations, dysphoria and paranoid delusions. Sometimes there can be a brief psychotic episode that lasts several hours to a couple of days.
chronic: Heavy long term cannabis use especially when started at an early age is associated with the development of schizophrenia (It is unknown whether this is a causal or correlational effect.), depression, suicidal thinking, severe lack of motivation, chronic hallucinations, and chronic dysphoria. In addition, dependency develops in about 9% but the withdrawal phenomena are mild.
Cognitive effects
acute: Cannabis impairs attention, short term memory, working memory, episodic memory, and psychomotor performance. In general, performance is slower and more clumsy but, unlike alcohol, individuals have an awareness of the impairment that causes caution as opposed to over-confidence.
chronic: There is no evidence to suggest that chronic low dose use of cannabis has any long term negative cognitive effects but there is evidence to suggest that chronic high dose use of cannabis may. Long term memory and other cognitive functions that are impaired with acute cannabis use should theoretically be impaired with chronic heavy use due to the fact that the brain usually adapts to the constant presence of exogenous molecules that bind to receptor sites for an analogous endogenous molecule. Also, theoretically, this effect should be more severe in an individual who begins heavy use during the time when his or her brain is still developing (prior to the age of 24). Making matters worse, again theoretically, is the fact that the pre-frontal cortex is filled with endocannabinoid receptor sites and is the last part of the brain to finish developing. However, there is not adequate research to fully answer these questions.
My guess is that we will someday find that occasional recreational use of cannabis has no long term cognitive effects but chronic daily use over many years reduces IQ and causes memory and other cognitive dysfunction that persists upon cessation and this is worse in people who begin heavy use during childhood.
Driving
Cannabis can impair the operation of heavy machinery and driving is not recommended while acutely intoxicated. The impairment causes behavioral inhibition. Things slow down and people tend to be more cautious. They also tend to be more clumsy. People who are intoxicated on cannabis have difficulty driving an obstacle course but they realize they are having difficulty and proceed much slower. Often times people don't desire to drive when acutely intoxicated on cannabis.
When people drink alcohol they feel invincible. They often want to drive and over-estimate their ability to drive. With alcohol there is behavioral dis-inhibition and lack of awareness of being impaired.
The most reliable studies to date do not demonstrate that cannabis increases the risk for a driver to crash his or her vehicle. This research is difficult to do because the primary measure is usually a positive blood level of THC. There is no way to know what percentage of these individuals were acutely intoxicated on cannabis alone at the time of the crash. Acute intoxication lasts hours and a positive blood level lasts weeks. Data from controlled studies done on a test track reveal impairment in driving ability. It is my belief that acute intoxication could cause an individual to be involved in a crash but to a significantly less degree compared with alcohol.
A close friend and fellow physician who is a long time daily user told me, "I have driven my car on numerous occasions while intoxicated on marijuana. I can tell you that my senses were impaired and I could have wrecked but I never did. I would not advise anyone to drive while impaired."
I asked if there might be a difference between a naive user and a chronic user. He said, "Yeah, I am sure that a naive user would be at much greater risk of crashing. The chronic user has more practice having an altered state of mind but is still impaired."
SECTION III
Medical uses
Probably real:
Chemotherapy side effects and AIDS - Cannabis causes reduced pain and nausea and increases appetite which can help a patient who is taking chemotherapy or who has AIDS. However, other medications are more effective, more reliable and have more predictable duration of action and potency.
Pain is managed with NSAIDs, Acetaminophen, opioids, antidepressants, and antiepileptics. Nausea is managed with 5-HT3 antagonists, dopamine antagonists, NK1 antagonists, antihistamines, benzodiazepines, anticholinergics, and steroids.
Appetite can be stimulated with 5-HT2C receptor antagonists/ inverse agonists, H1 receptor antagonists/inverse agonists, dopamine antagonists, adrenergic antagonists, corticosteroids, pregnene steroids, anabolic steroids, sulfonylureas, pregabalin, and Insulin.
Pain and nausea both respond well to placebo treatment and to hypnosis. Any non-traditional therapy such as acupuncture, homeopathy, chiropractic care, etc. can effectively treat pain and nausea. In other words, suggestion can treat pain and nausea.
Cannabis induced increased appetite is not associated with weight gain so I am confused as to whether this would help an AIDS or cancer patient to gain weight. Maybe it increases the efficiency of the digestive process and causes your body to move towards your genetically designed weight. That would mean that a chemo patient would get back to his normal weight and then not keep gaining. I am not sure that is the case but that would be my guess.
Epilepsy- Dravet syndrome is a rare childhood illness that causes intractable seizures that are minimally responsive to anti-seizure medications. Cannabis that is high in cannabidiol (CBD) and low in THC stops these seizures. It is administered in liquid form to small children. They experience no high but their seizures, which can be up to 300 per day, become something like once or twice per week. This has only been discovered recently and is undergoing intense research at this moment. There is little evidence that cannabis is effective for the majority of common seizure disorders but there may be other rare forms of epilepsy such as Doose syndrome, Lennox-Gastaut syndrome and childhood idiopathic epilepsy that could respond to CBD. For more information go to this website: Epilepsy Foundation Calls for Increased Medical Marijuana Access and Research.
Glaucoma- Cannabis does reduce intra-ocular pressure but the potency and duration of effect are unreliable and it is difficult to have effective blood levels 24 hours per day. Prostaglandin analogs and beta-adrenergic antagonists are the first line treatments for glaucoma. These medications are not indicated for some people due to side effects but there are plenty of effective alternative treatments including adrenergic agonists, carbonic anhydrase inhibitors, parasympathomimetic agents, and osmotic agents. Marijuana in the Treatment of Glaucoma CTA - 2013 Jun 2013, AAO Complementary Therapy Task Force, Hoskins Center for Quality Eye Care, The American Academy of Ophthalmology
Multiple Sclerosis (MS)- Cannabis can reduce spasticity in patients with MS according to several placebo controlled studies. Sativex (Nabiximol) is a THC/CBD combo medication that will likely be FDA approved in the near future and has demonstrated efficacy in the treatment of spasticity in MS. However, baclofen, valium and botox are the first line treatments. Muscle stiffness, body pain, spasms and sleep quality also improve with cannabis.
I have MS and I may occasionally consume marijuana recreationally but I would not want to consume it on a regular basis. My cognitive function is very important to me. I might think differently if I had severe spasticity that was unresponsive to other treatments. The problem is that MS patients have cognitive problems that can be made worse with cannabis. This has been confirmed in several placebo controlled studies.
Alternatively, if the high CBD form of cannabis or some other single component of cannabis that has been made into pill form turns out to be helpful for sleep and/or spasms without cognitive effects I would be very inclined to use it daily. Or, maybe there is a specific named strain of cannabis that you can buy at a dispensary that is low in cognitive impairment and high in sleep induction and spasm reduction.
I certainly encourage research on this but I am hesitant to make wild claims right now. By "research" I include me running around to different dispensaries and investigating all the strains. I will let you know what I find. National Multiple Sclerosis Society- Marijuana
Neuropathic pain- (AIDS, MS, diabetes, trauma, post surgery)- Neuropathic pain is pain resulting from injury to the central or peripheral nervous system. Several placebo controlled trials demonstrate consistent findings that neuropathic pain is reduced in a dose related fashion with cannabis administration. Neuropathic pain is difficult to treat so an additional medication would be welcome, however, achieving a 24 hour per day therapeutic dose of cannabis over a long period of time and in a reliable way is difficult. Also, there are deleterious effects of the cannabis when used long term and at high dose. Tricyclic antidepressants would be the treatment of choice and there is no evidence that cannabis would have greater effectiveness or efficacy. Other treatments include gabapentin, lamotrigine, and SSRIs.
Maybe real:
Cancer- Studies in mice and rats have shown that cannabinoids other than THC may inhibit tumor growth by causing cell death, blocking cell growth, and blocking the development of blood vessels needed by tumors to grow. Laboratory and animal studies have shown that cannabinoids may be able to kill cancer cells while protecting normal cells. Specific types of cancer that cannabinoids have shown effectiveness in treating in vitro and in animal models include: liver, colon, non-small cell lung, breast, and glioma. However, there are no good studies that demonstrate efficacy in real human tumors.
Diabetes Type II- There is not enough research yet but cannabis does lower fasting insulin levels and improves carbohydrate metabolism. Despite getting the "munchies" cannabis users tend to be less obese. Marijuana: The next diabetes drug? Maia Szalavitz, Time.com, CNN Health News
Auto-immune illness- Cannabinoids have been found to suppress the immune system presumably through the CB2 receptor which is found peripherally and has recently been found in limited locations in the brain. This is a double edge sword as immune suppression might be good for some auto immune illnesses such as Lupus, and I hope MS, but bad for infections and certain tumors. Clinical research in humans is neededAlzheimer Disease- Some preliminary in vitro data indicate a possible role for THC in reducing a specific type of malformed protein associated with Alzheimer disease. If the impediments to our ability to study this can be lifted we should be able to find out if THC can delay the progression in Alzheimer disease without causing negative cognitive effects. I would not want to risk making short term memory worse in a patient with early Alzheimer disease unless it was for a good reason. Since we are years away from having these answers I would not advocate smoking cannabis in a chronic fashion in order to treat Alzheimer disease at this time.
Maybe, maybe some real symptomatic benefit:
ALS, Huntington's Chorea, Parkinson's disease, Tourette Syndrome and Migraine headache
Probably not real:
Alcoholism, amyloidosis, anorexia, ADHD, autism, Crohn's disease, depression, and any list that includes every illness under the sun.
*Possibly dangerous:
Bipolar disorder, Schizophrenia, anxiety conditions such as OCD and Panic disorder, and PTSD
*There are no prospective double blind studies in humans that demonstrate the efficacy of cannabis in the treatment of these conditions. I have personally seen individuals with these conditions who have had "bad trips" with cannabis use and there are a number of cannabis side effects that would make cannabis a less than ideal drug for these conditions. Alternatively, some preliminary research suggests that the endocannabinoid system may be involved in anxiety and that cannabis may have a short lived effect at reducing anxiety. My take is that cannabinoids may have a role in anxiety reduction for use in these conditions but we are years away from having this knowledge. I also think there may be a dose response issue where higher doses of cannabis cause anxiety while lower doses relieve anxiety. I would not currently advise anyone to use cannabis purchased at a dispensary for the purpose of treating one of these conditions but if you are a recreational user who has some ordinary anxiety you can most likely find strains that have an anxiolytic effect.
Pharmacology
Most cannabinoids are fat soluble. For heavy users who have saturated their fat stores this produces a lengthy half-life while these chemicals slowly leech back into the blood stream to be metabolized and eliminated. For less frequent users cannabis moves from the blood stream into fat stores making the half-life significantly less compared with heavy users.
In a naive user THC is detectable in the blood stream for 3 to 10 days but heavy users can produce a positive blood test for up to 3 months.
The psychoactive effect is immediate when smoked and delayed by 30 minutes or more when ingested orally. The duration of action when inhaled through the lungs may be up to several hours and when digested in the stomach may be longer.
Individuals whose fat stores are saturated have faster, stronger and more sustained effect. Sometimes in these individuals THC may leech into the blood stream to cause a psychoactive effect when there has been no recent oral intake. This is called a "flash-back."
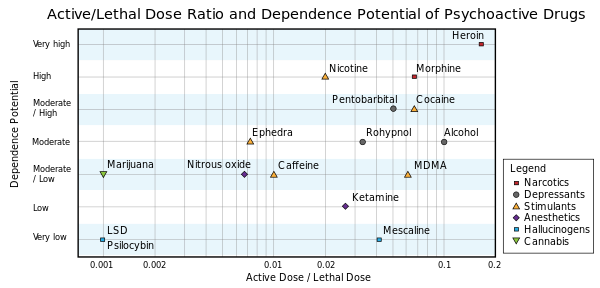
Lethal toxicity is very low and there are no recorded deaths directly from cannabis overdose. (Deaths can occur secondary to a brief psychotic episode while acutely intoxicated in individuals who are predisposed but there are no reports of death due to a toxic pharmacologic effect.)
Acute symptomatic toxicity is common. All the acute somatic, psychiatric and cognitive symptoms can be more severe if too much cannabis is ingested. Overdose can easily occur by mistake because it is usually hard to be sure of the exact potency of the cannabis. Also, naive users may be unfamiliar with the pharmacology.
Cannabis contains more carcinogens than does tobacco smoke. The reason it may be significantly less problematic in regards to lung cancer is due to the way it is smoked. Two or three hits of cannabis may get you high for several hours whereas it takes two or three packs of cigarettes every day to keep a tobacco addict feeling good.
Biochemistry
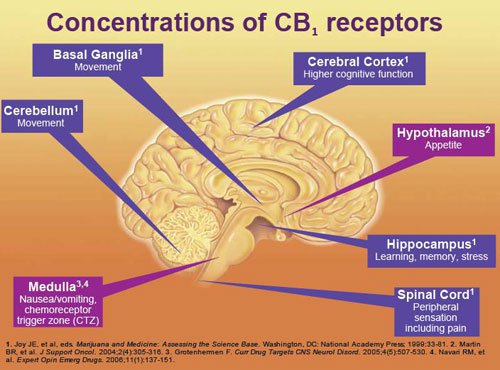
The endocannabinoids anandamide, 2-arachidonoyl-glycerol (2-AG), palmitoyl-ethanolamide, docosatetraenylethanolamide, homo-gamma-linoenylethanolamide, and oleamide are produced in post-synaptic neuronal cell membranes when regulatory neurotransmitters such as dopamine, acetylcholine, serotonin, etc. stimulate their respective post-synaptic receptor sites. These endocannabinoids then go backwards to the pre-synaptic neuronal membrane to stimulate the cannabinoid (CB1) receptor. The endocannabinoid system modulates or regulates the neurotransmitter systems that modulates or regulates bodily functions.
For example, in the hippocampus there is a neurotransmitter called acetylcholine that functions in the process of laying down new memory. It is produced in a pre-synaptic neuron and travels to a post-synaptic neuron where it attaches to a receptor that regulates the main neurotransmitters which are GABA(-) and glutamate(+). An endocannabinoid such as anandamide then provides feedback inhibition that regulates the acetylcholine.
CB1 receptors are in higher number in certain locations in the brain. These locations correlate to physiologic action. In the hippocampus we know that exogenous cannabinoids such as THC effect short term memory. We think this is due to their effect on the CB1 receptor in the hippocampus.
Most medicines that affect the brain mimic neurotransmitters that function in the forward direction for direct stimulation or inhibition (direct regulation of GABA and glutamate). Endocannabinoids function in a backwards fashion to regulate these regulatory neurotransmitters. It is thought that exogenous cannabinoids such as THC flood this system and de-couple this regulatory function resulting in too much inhibition.
The endocannabinoid receptor CB2 is found in the immune system and functions there in a similar fashion. Recently, we have discovered a limited number of CB2 receptors in the central nervous system which provides hope that perhaps brain illnesses that are associated with an inflammatory process may respond to cannabinoid therapy. So far we have discovered no additional cannabinoid receptors but most researchers believe there are other receptors involved.
By understanding the function of the endocannabinoid system we can understand the effect of exogenous cannabinoids on the human body. This research is still in its infancy.
Research issues
Research on cannabis has a very unusual history.
The Marijuana Tax Act of 1937 was passed by the federal government because the federal government could not regulate medications at that time. This was a state responsibility. The federal government wanted to make cannabis illegal nationwide so they constructed the legislation to effectively make it so.
Making cannabis practically illegal killed the ability of anyone to do research. University professors could not obtain it. Thus, unlike many other compounds, cannabis has undergone very little scientific research in the past 75 years. Actually, the government did some research but I think most would agree they had a bias. They only looked for negative or harmful things.
Cannabis laws should be changed and our current laws make no sense but in the past the actions that were taken were not unreasonable. I believe that our leaders honestly believed it to be a harmful drug of addiction. Proponents of legalizing cannabis frequently distort this history for the purpose of making the argument that there was no rational explanation for making it illegal in the first place. I do not agree with that assessment.
One argument is that cannabis has been used for thousands of years as a medicine and in the 18th century it was widely used for its medicinal effects. Therefore, the 1937 legislation must have been a devious plot by people who had ulterior motives.
If you look at the history of medicine you will see that there are lots of compounds that have been used for thousands of years and there are lots of compounds that were used as medicines in the 18th century. The majority of these are not currently FDA approved.
If you look around today you see thousands of medications in the alternative and holistic markets that are no better than placebo. Remember, all fake medicines can work to produce compensatory physiologic effects such as pain reduction, anti-nausea and perhaps sleep induction and a few other things through the effects of suggestion. These effects are then falsely transformed into claims that a particular treatment cures all kinds of things including cancer. For many reasons, including profit, this is what people do. Placebo medicine has a rich tradition in human history. If you want to read more about this go to: Placebo Medicine by Morgan Levy, MD.Have you ever heard of a "snake oil" salesman?
The reason the FDA exists is due to the 18th century practice of making money by selling fake medicine. A practice that we are still fighting today, by the way. For whatever reason, humans are very susceptible to someone who is selling a product that is claimed to heal something. Here is one example.
There is a water snake called the Erabu that lives off the coast of China. Its oil is particularly high in prostaglandins and it was used to sooth arthritis and sore muscles in China. Some of this oil made it to America when a large number of Chinese came here. A lot of these immigrants worked building railroads and this "snake oil" became popular. Unfortunately, the erabu did not live here. No one knew that different snakes have different compounds in their oil. No one knew what a prostaglandin was because it had not been discovered yet. Charlatans began going around the country selling rattle snake oil as an elixir that they claimed would cure almost anything. When rattle snake oil was not available they would sell any oil they could find and just call it "snake oil." This was legal because there was no FDA.
Re-read the medicinal uses section in this essay and tell me with a straight face that in 1937 we knew that cannabis would help with these conditions. Even the current medicinal use for cannabis is relatively limited compared to the claims that it cures everything. Factor in the affective and cognitive impairment that acute intoxication causes and the brief psychotic episodes or "bad trips" that occur and the outlawing of cannabis in 1937 does not seem that unreasonable. (I will cover the arguments with regards to hemp in a later section entitled "Hemp.")
Fortunately, there is now a boom in research on cannabis. This is fueled by the very recent finding that intractable childhood seizures associated with Dravet syndrome are remarkably controlled with cannabis that is high in cannabidiol and low in THC. It is also fueled by the positive effect that cannabis can have on neuropathic pain and spasticity. There is also the finding in vitro and in animal studies that there may be some cancers that respond positively to cannabinoids and maybe even some auto-immune illnesses.
Cannabis is not helpful for the vast majority of seizure disorders and there is only a small amount of evidence to suggest it may help with some cancers but now Colorado is inundated with people coming in search of a cure for all kinds of things. People are desperate and they ignore their doctor's advice and they think the government is tricking them. In my opinion, we need to study this for five minutes and find out what is real.
Some of the stuff the government was saying about cannabis was untrue including the infamous Reagan era study. Nevertheless, I do not believe that there was a widespread conspiracy to defraud the public. I truly believe that Reagan believed that cannabis was a harmful substance and that he was protecting the public by limiting access to it.
An additional problem with cannabis research is that the strains of available cannabis to study vary considerably from place to place. When you study a drug, such as aspirin, you isolate some salicylic acid and everyone who studies aspirin obtains some and then we are all studying the same single compound. This has been hard to do with cannabis. There is a government farm but what it makes is different from what you might find on the street in East LA. There are 60-70 active compounds in cannabis and some evidence to suggest that a synergistic effect is needed for certain types of treatments. Needless to say, there is a lot of work to do to figure out everything that is true, or not true, for the medical uses of cannabis.
In conclusion, research is a way of assessing a phenomena in which you use logic to investigate all possible explanations with adequate controls to prevent bias. I am irritated that this process has not been allowed to proceed with cannabis. I am equally irritated that so many people bypass this process and proclaim all sorts of medical benefits for cannabis without reliable evidence.
SECTION IV
Legal issues
There is one nation on planet Earth where cannabis is outright legal. Uruguay legalized cannabis on Dec. 10, 2013.
Although the states of Colorado and Washington made cannabis legal in 2014, the United States did not. President Obama has said that the federal government will not intervene inside the borders of Colorado and Washington.
States all across America and nations all around the world are moving in the direction of legalization although they are hesitating at this moment in order to observe how the experiment is working in Uruguay, Colorado and Washington.
The only other places where it is kind of legal are the Netherlands, Bangladesh, and maybe North Korea.
World Map of Cannabis Legality
Laws concerning cannabis vary greatly from nation to nation. In some nations it is legal to possess small amounts or to consume it in certain locations. In other nations, possession of cannabis can result in a lengthy jail term (4 years for possession in Indonesia) or in capital punishment (execution for possession of 500 grams in Singapore).
When a legal offense is justified it tends to garner similar laws everywhere. When laws vary greatly across the globe it is usually because the law is of questionable justification. That is my personal observation.
In today's world there are many places where cannabis might be fully legal except that in 1961 most nations signed on to the Single Convention on Narcotic Drugs. This was an international treaty to make all illicit drugs illegal. Cannabis probably should not have been included based on what we know today. When Uruguay made cannabis legal they were violating this treaty and testing international resolve to enforce it. Other countries are waiting to see how this pans out. If nothing happens to Uruguay, I predict that a number of countries will legalize cannabis.
Social issues
You will see a lot of information about the social impact of cannabis in the literature. I dredged though a ton of it. The general trend is that these articles might be correct in detail but are usually incorrect in the big picture. Here is an example: "Cannabis has been shown to affect your coordination so it will cause you to crash your car and kill someone." The premise is accurate but the overall conclusion ... not so much.
This example of taking a bit of information and applying it inaccurately repeats itself over and over in government literature.
Claims I have read include:
"Marijuana causes low achievement in high school and college."
"Marijuana causes delinquent behavior."
"Marijuana causes aggression, rebellion, and poor relationships with family, especially parents."
"Marijuana caused 17% of treatment admissions in the US in 2008."
"Marijuana is smoking and smoking causes cancer."
"Marijuana lowers your IQ permanently."
"Marijuana will make it impossible to get a job as all employers do drug tests."
"Marijuana will affect your communication and cause you to sound dumb."
"Marijuana use leads to use of cocaine and heroin."
"Marijuana use causes mental illness."
"Marijuana will lower your sperm count."
The list goes on and on. Like I said, these statements may have some truth to them but the inference they make is almost always incorrect.
Sometimes, it can be a dose issue. Heavy chronic users have been shown to have some lung damage, reduced testosterone, low sperm count, possible permanent IQ changes, and low motivation and life achievement. However, this has never been demonstrated in a mild to moderate user. It is amazing to me the number of anti-cannabis articles (many made by the government) that I saw that do not differentiate between use and abuse. It would be like saying, "If you drink an occasional glass of wine with dinner you will get cirrhosis of the liver."
It can be a correlation vs cause-effect issue. Smoking cannabis is correlated with an incidence of schizophrenia but there is little reliable evidence that there is a causal relationship. In my professional opinion, cannabis most likely unmasks symptoms of a pre-existing condition. Nevertheless, lots of literature proclaims that cannabis causes schizophrenia.
I was amazed when I saw that 17% of admissions to drug dependence treatment facilities was for cannabis. I later learned that the overwhelming majority of these admissions were not voluntary. Criminals who have THC in their blood are often able to reduce a sentence for whatever crime they committed if they agree to go to a drug treatment facility. I am thinking that if you are a criminal you should always maintain some THC in your blood so you will have this out when you appear in court.
There are numerous issues like these. I suggest that when you hear a claim about cannabis you maintain some doubt until you have a chance to get the whole story.
Here is my overall take on the social impact of cannabis:
As long as there is an illegal industry there will be a negative social impact from cannabis.
If cannabis was fully legal everywhere there would still be some negative impact.
There can be a negative psychiatric effect on individuals who suffer a psychotic disorder such as bipolar disorder or schizophrenia or who have an anxiety condition such as panic attacks.
Alternatively, more widespread acceptance and use of cannabis could reduce tobacco and alcohol use reducing the negative effects to society from those drugs. (Remember that you should not do both at the same time as I did.)
The scare tactics used in the past such as saying, "Cannabis use will destroy the very fabric of society," are funny. These statements now belong in the history books.
The claims about medical use have been greatly exaggerated on the one hand but severely understudied on the other hand. It is hard to tell at this time how great of an impact cannabis will have from a medical perspective.
Long term chronic abusers may impact the health care system due to lung disease, cancer and other problems but not on a scale comparable to tobacco and alcohol.
Driving is an issue but nothing like it is with alcohol.
The lack of motivation and cognitive changes in chronic users may have societal ramifications if their numbers increase dramatically after legalization.
If the strain of cannabis that can now be legally grown for hemp in Colorado and Washington turns out to be a wonder material that would certainly be a great thing for society but the claims so far have been inflated. (see the next section on Hemp)
In regards to the monetary cost to society we know that alcohol and tobacco cost a lot more than they bring in. I believe that the overall income to the government from taxation of cannabis will be far greater than the overall economic impact from people using it. That is a guess and we will have to see how the experiment turns out.
One issue that I feel strongly about is education. People need some basic education about cannabis. Most sources are heavily biased. Perhaps, people who know a lot about substance abuse and brain science should write articles that are 98% un-biased. Ya think?
SECTION V
Hemp
Hemp is cannabis that is low in THC and high in fiber content.
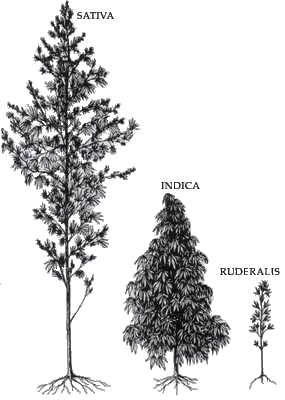
There are three subspecies of Cannabis sativa:
1. Cannabis sativa sativa
2. Cannabis sativa indica
3. Cannabis sativa ruderalis
The three subspecies are all the same species so they can interbreed but they have varying amounts of fiber, CBD, THC and everything else. Farmers have produced numerous new subspecies that we call strains for the purpose of increasing the yield of whichever effect they desire.
Hemp is refined into products such as hemp seed foods, hemp oil, wax, resin, rope, cloth, pulp, paper, and fuel. There are numerous products that can be made from hemp. To view more of these products go to this website: Hemp.com
As a food, hemp is a good source of protein. Numerous products are now available including milk, seasoning, beer, salads, cereals, waffles, ice cream, tofu, nut butters, etc. Since 2007 the market has improved but it is unknown what the market potential will be. The most reliable estimates, in my opinion, project that it will remain a relatively small market similar to sesame and poppy seeds.
As a fiber, hemp has a long history. Today there is a modest current industry in making clothing, ropes, paper, etc. Pure hemp has a texture similar to linen. The word "canvas" is derived from the word cannabis. Most ropes used on ships used to be made from hemp but they would frequently rot and required tarring which was expensive and labor intensive. Manila was better and largely replaced hemp as a fiber for rope. Today there are numerous fibers that are used but nylon is clearly the best.
Hemp has been used for paper but it is expensive to process and not significantly better than wood fiber. Hemp paper is currently a small niche market.
Cannabis plastics and building materials have been put in homes and automobiles. Biofuels have been produced using cannabis oil. The cost effectiveness and competitive advantage of using hemp is yet to be fully determined. Currently this is a limited market. It might have tremendous potential but who knows?
Similar to the problems associated with medical research, the research and development of hemp products has been limited secondary to the Marijuana Tax Act of 1937. Thus, there is a lot we do not know about the commercial viability of Hemp.
Hemp has many uses and some may create a large market but many will only support a limited market. There are many fibers, foods and oils in the marketplace and they all have their advantages and disadvantages. Hemp is no different. Despite the unusual legal history of cannabis, I believe that market forces will primarily shape the industrial use of hemp.
We are about to find out if I am right or not. The congress of the United States finally made hemp sort of legal. Buried in the $956 billion farm bill is an amendment, co-sponsored by Rep. Massie, that legally distinguishes industrial hemp from marijuana after decades of conflation. It defines hemp as an agricultural crop rather than a drug. This effectively frees American farmers to grow it for the first time in almost 60 years. The hemp that is now a farm product is a specific strain of cannabis sativa that is low in THC content. It would be worthless on the marijuana market. This was reported in an excellent article by Rolling Stone magazine.
It will only be legal in states where cannabis is legal. Colorado farmers will be the first Americans to plant hemp for commercial purposes since 1950.
I suspect that at least a few hemp products could be huge money makers but it is hard to be sure which ones.
Finally, the popular notion that hemp was made illegal to protect certain markets from competition is probably not accurate. These are modern claims that are probably examples of historical revisionism.
If I am wrong, how do you answer these questions:
-How much THC was in a typical strain of hemp in 1937 and were politicians fearful it would be smoked?
-Don't you think lawmakers probably feared that individuals would skirt the law if hemp, which is cannabis sativa, remained legal?
-The twenties and thirties were the heyday of modern materials made in chemistry labs. They loved these new materials back then and saw them as the future. Hemp was an old fashioned plant with numerous downsides. It was not the wonder plant with 250,000 uses that cannabis activists promote today. Do you really think that the idea of making hemp illegal in order to curtail illicit drugs was viewed then as it is now?
-Just because hemp production was promoted to help in WWII does not mean that it was going to be competitive in the marketplace for things like food, paper or Biofuels. Do you really think that hemp rope could compete with nylon rope?
It is hard to look at an historical event and remember everything that was happening, or that people were thinking, at the time. The people who are making these claims are not people who want to wear a hemp T-shirt or read a paper written on hemp. They are people who want to be able to freely smoke cannabis for personal pleasure. When you really research this issue it is hard to find clear historical evidence that there was intentional or malicious behavior going on. That is my opinion.
Conclusions
Cannabis consumed in chronic high dose has harmful health effects.
Cannabis consumed in chronic low to moderate dose has no harmful health effects and may have some beneficial health effects.
Cannabis can be useful for some medical conditions but the extent to which it is useful has been greatly exaggerated. Dravet Syndrome is a rare childhood seizure disorder that appears to be treated remarkably well with cannabis that is high in cannabidiol and low in THC. There may be other conditions for which a cannabis component may be a first line treatment but, in general, things like glaucoma, appetite, pain, muscle spasms and nausea are better treated with other medications.
For some individuals who have an underlying anxiety or psychotic condition cannabis may induce a brief psychotic episode or "bad trip" causing harm to self or others. However, low doses of certain cannabinoids may have a role in the treatment of mild anxiety.
About 9% of cannabis users will develop long term addiction but the withdrawal syndrome is mild.
There is no risk of death directly from toxic effects of cannabis but death may rarely occur secondary to a cannabis induced brief psychotic episode.
Driving is impaired while acutely intoxicated but there is no current evidence that cannabis is responsible for significant numbers of motor vehicle accidents.
Cognitive changes occur with acute Cannabis intoxication. These changes resolve on cessation. There is no evidence that chronic moderate use causes permanent changes. There is some evidence that chronic heavy use, especially when begun prior to the age of 24, may cause permanent or at least semi-permanent cognitive change.
Cannabis has been poorly researched due to a number of issues but this has now changed. Going forward there are sure to be more FDA approved medications as well as hemp based products that come from cannabis constituents.
Finally, legal and social issues need to be discussed and resolved so that there can be more sensible public policy in regards to cannabis.
Addendum-
How to safely consume cannabis:
If you are a naive user and you choose to ingest cannabis I would suggest that you smoke it rather than eat it so you will know immediately how it is effecting you. Don't have any other mind altering substances in your body at the same time. Only take one or two hits. Know the potency of the cannabis and smoke it with someone who is experienced. Try to smoke cannabis that is less than 15% THC. Less than 10% would be even better for a naive user. Don't smoke it alone. Smoke it at ground level. Don't drive afterwards. Don't have knives or guns laying around. Plan on being at home and going to sleep afterwards. Don't do it if you have a heart condition, anxiety disorder, psychotic illness or if you are someone who has difficulty letting go of control. You don't need to inhale deeply and hold it as many users do. You can inhale and exhale gently as you would with a cigar and you will achieve the same blood level. The effect should have immediate onset and last from 30 minutes to a couple of hours. Be prepared to have an altered state of mind and a feeling of lack of control. Try to lay back and enjoy the experience and do not fight it.
I hope that this essay has been useful.
-Morgan Levy, MD









{kind=link}